Depression does not always look like visible sadness. In many cases, it shows up as shutdown: avoiding tasks, canceling plans, isolating, and feeling unable to act even when you understand what needs to change. That is one reason some people do not improve enough with insight-based weekly therapy alone. This guide explains when DBT may help, which depressive patterns it tends to fit best, and when a higher level of support, such as IOP or PHP, may be more appropriate.
Depression does not always look like visible sadness. In many cases, it shows up as shutdown: avoiding tasks, canceling plans, isolating, and feeling unable to act even when you understand what needs to change. If weekly therapy has helped you make sense of your depression but hasn’t changed the pattern, you’re not alone, and the issue may not be effort or insight. It may be that the approach needs to shift.
Is DBT Effective for Depression?
Yes, but for specific presentations. DBT is most effective for depression that involves emotional reactivity, chronic avoidance or withdrawal, difficulty using coping skills in real life, or patterns that haven’t responded to traditional talk therapy alone.
Unlike standard talk therapy, DBT combines weekly individual sessions with group skills training, homework practice, and (in comprehensive programs) phone coaching between sessions. The skills target behavior change directly, not just insight, which is why it can break cycles that other approaches leave intact.
A clinical evaluation is the most reliable way to determine whether DBT is a good fit for your specific symptoms and level of functioning. Further in this guide, we outline exactly what clinicians assess, what the first weeks of depression treatment look like, and when a higher level of care, such as IOP or PHP, may be the better starting point.
How DBT Differs from Traditional Talk Therapy for Depression
Dialectical Behavior Therapy (DBT), originally developed by Dr. Marsha Linehan, is built on one core idea: change and acceptance have to happen at the same time. Instead of focusing only on insight, DBT teaches skills that you actively practice between sessions.
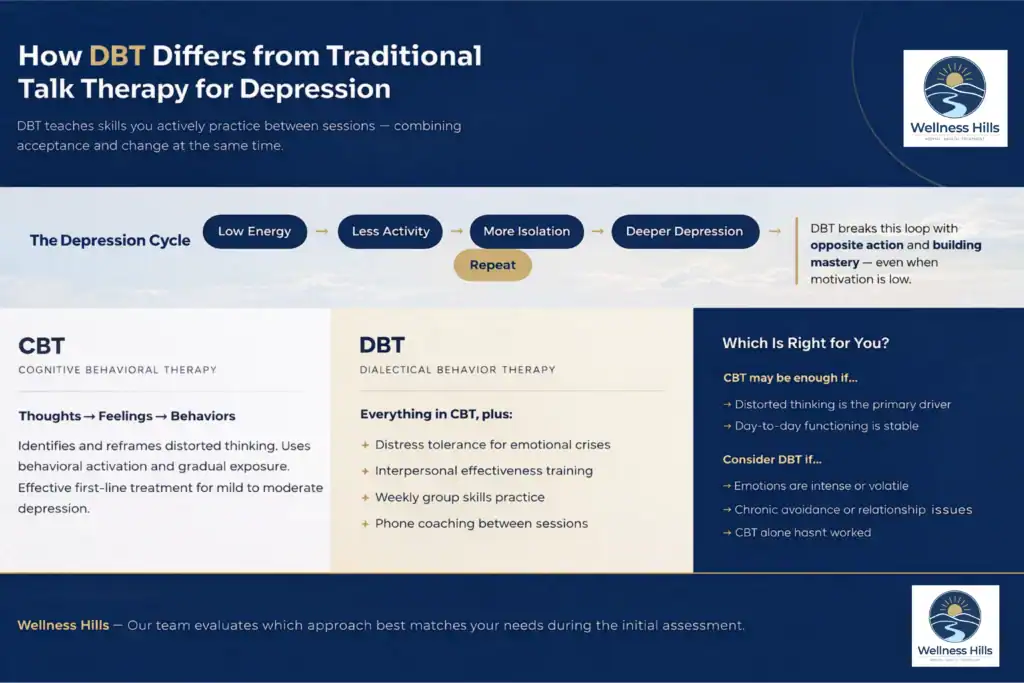
How DBT Uses Behavioral Activation to Break the Depression Cycle
In many cases, depression isn’t just about negative thinking; it’s about behavioral shutdown.
- You stop going out
- You cancel plans
- You avoid tasks
Over time, that creates a loop:
low energy → less activity → more isolation → deeper depression.
Standard therapy, including CBT for depression, often focuses on thought patterns. That’s important. But for some people, insight alone doesn’t break the cycle.
DBT interventions generally directly target behavior using structured techniques like opposite action and building mastery, skills that push against withdrawal, even when motivation is low.
DBT vs. CBT for Depression: What DBT Adds
CBT and DBT are not competing therapies; they share a foundation. Both are structured, skills-based, and backed by strong clinical evidence for treating depression. The difference is in emphasis and format.
Where CBT focuses: CBT targets the relationship between thoughts, feelings, and behaviors. It uses techniques such as cognitive restructuring (identifying and reframing distorted thoughts), behavioral activation (scheduling activities to counteract withdrawal), and exposure (gradually facing avoided situations). For many people with mild to moderate depression, CBT alone is effective. Research supports CBT as a first-line treatment.
What DBT adds: DBT was built for people whose emotions are more intense, more volatile, or harder to regulate than what standard CBT was designed to address. It adds four components that CBT typically does not include:
- Distress tolerance skills – structured techniques for surviving emotional crises without making them worse, which matters when depression produces urges to withdraw, self-harm, or use substances
- Interpersonal effectiveness training – specific frameworks (like the DEAR MAN and FAST acronyms) for communicating needs and maintaining self-respect in relationships, which is critical when depression erodes social functioning
- Group skills training – a weekly group format where skills are taught, practiced, and reinforced with peers, which provides accountability and normalization that individual therapy alone cannot replicate
- Phone coaching between sessions – in comprehensive DBT programs, therapists are available for brief between-session calls to help apply skills in real time during a crisis
When CBT may be the better fit: If your depression is primarily driven by distorted thinking patterns (catastrophizing, all-or-nothing thinking, personalization) and you’re functioning reasonably well day to day, CBT may be sufficient. If your depression involves emotional volatility, chronic avoidance, relationship dysfunction, or has not responded to a full course of CBT, DBT may address the gaps.
At Wellness Hills, our clinical team evaluates which approach or combination best matches your presentation during the initial assessment.
Core DBT Skills Used in Depression Treatment
This is where the DBT skills for depression become practical. Each skill targets a specific pattern.

1. Opposite Action: How It Interrupts Depressive Withdrawal
Depression often creates urges that feel logical, but make things worse.
You feel low → you want to isolate → isolation deepens the mood.
That loop reinforces itself. The opposite action is designed to interrupt it.
When teaching DBT techniques, the opposite action is often used in two cases:
- When the emotion doesn’t match the facts
- Or when acting on the emotion would make the situation worse
In both cases, you act opposite to the urge:
- Going to the event you want to cancel
- Starting the task you’ve been avoiding
It often feels forced at first. That’s expected. But over time, this shifts behavior first, and mood follows. Instead of reinforcing withdrawal, you begin to weaken it. And that’s what starts to break the cycle that keeps depression in place.
2. Mindfulness in DBT: Interrupting Rumination Before It Deepens
Depression pulls attention into:
- Past regret
- Future worry
Mindfulness in this context is not abstract. It’s specific:
- Observe what’s happening
- Describe it in words
- Participate in the present moment
This helps you catch rumination earlier, before it pulls you deeper.
3. Emotion Regulation: The ABC PLEASE Skills for Depression
This is where DBT becomes preventive, using the ABC PLEASE skills to reduce emotional vulnerability and build resilience.
According to clinical training protocols and research published by the National Institutes of Health (NIH) and the Behavioral Tech/Linehan Institute, these techniques serve as biological and emotional buffers. Instead of waiting for motivation to arrive, you use these structured actions to build it from the ground up:
- A – Accumulate Positive Emotions: Actively seeking short-term pleasant activities and working toward long-term life goals to build a life worth living.
- B – Build Mastery: Doing at least one thing daily that makes you feel competent and effective to combat helplessness.
- C – Cope Ahead: Rehearsing a plan in advance for situations that you know will be emotionally challenging.
- PLEASE – Reduce Physical Vulnerability: Taking care of the body to support the mind through:
- PL: Treat Physical iLlness
- E: Balanced Eating
- A: Avoid mood-Altering substances
- S: Balanced Sleep
- E: Regular Exercise
Depression often includes anhedonia (loss of interest). These skills rebuild engagement by focusing on actions first. By accumulating small wins and managing physical health, you gradually lower the activation energy required to feel positive emotions, even before natural motivation fully returns.
4. Check the Facts: A Structured Skill for Challenging Depressive Thinking
Depression doesn’t just affect mood; it shapes perception. A single email from a manager can become: I’m going to lose my job.
Check the Facts is a structured process for evaluating whether your emotional reaction matches the reality of the situation.
Check the Facts creates a structured pause:
- What actually happened?
- What evidence supports this thought?
- Are there alternative explanations?
This isn’t about forced positivity. It’s about accuracy.
Who is a Good Candidate for DBT? What Clinicians Assess
A common question: Am I the right fit for this?
Clinicians at Wellness Hills, such as Leigh Rasmussen, LPC, LCADC (Program Director), and Abby Goodrich, LAC (Primary Therapist), look for specific patterns when assessing whether this approach is likely to help. Here’s what they may pay attention to:
- Your depression comes with strong emotions or relationship stress, not just low mood
- You’ve tried therapy before, but it didn’t really stick
- You tend to avoid things, withdraw, or shut down
- You know coping skills, but you don’t use them in real life
- You struggle with self-worth, emptiness, or managing emotions
If this sounds familiar, DBT may be a better fit.
Not because it’s better than other evidence-based therapies, but because it focuses on changing patterns rather than just understanding them.
DBT therapy is not the right fit for every presentation. In many clinical settings, the following are common reasons to delay DBT in favor of more immediate interventions:
- Primary Psychotic Disorders: Conditions like schizophrenia often require specialized First Episode Psychosis (FEP) programs.
- Severe Cognitive Impairment: If a person cannot mentally participate in the complex load of activities and homework, standard DBT may be less helpful.
- Unmanaged High-Risk Behaviors: If a client’s immediate environment is so unstable that they cannot attend weekly individual and group sessions, Intensive Outpatient (IOP) or residential care is usually the first step.
Your DBT placement is based on what the assessment reveals about your symptoms, functioning level, and treatment history.
When Depression Includes Anxiety, Trauma, or Substance Use

Depression rarely shows up alone, especially at the IOP or PHP level of care. At Wellness Hills, many of the people we work with are managing depression alongside one or more co-occurring conditions. DBT’s modular skill set makes it particularly well-suited for these overlapping presentations.
Depression and anxiety: These two conditions share a common thread: emotional avoidance. DBT’s distress tolerance and opposite action skills target avoidance directly, making them effective for both the withdrawal of depression and the escape behaviors of anxiety.
If you find yourself canceling plans because of dread, avoiding phone calls, or spending hours in anticipatory worry before an event, DBT addresses both the depressive and anxious components of that pattern.
Depression and trauma: For people whose depression is rooted in or worsened by traumatic experiences, DBT provides a stabilization framework.
The distress tolerance module gives you tools to manage trauma-related emotional flooding without dissociating or shutting down, which creates the safety necessary to eventually process the trauma itself, either within DBT or through a complementary approach like EMDR or CPT.
DBT is often used as a first-phase treatment to build the emotional regulation capacity that deeper trauma processing requires.
Depression and substance use: Substance use and depression frequently reinforce each other: substances temporarily relieve depressive symptoms, but their aftereffects deepen the depression, creating a cycle. The ABC PLEASE skill explicitly addresses this by including Avoid mood-altering substances as a core vulnerability-reduction strategy.
If you are unsure whether your depression involves co-occurring conditions, that is exactly what the clinical assessment is designed to clarify.
Red Flags vs. Normal Discomfort: When to Step Up Your Level of Care
Growth in therapy is rarely comfortable. Understanding the difference between expected challenges and red flags helps determine if you need more support.
| Normal Discomfort (Expected) | Red Flags (May Need Higher Care) |
|---|---|
| Feeling emotionally tired after group sessions. | Consistent inability to attend sessions due to severity. |
| Noticing emotions more acutely via mindfulness. | Worsening passive or active suicidal ideation. |
| Temporary frustration that skills feel mechanical. | Increasing substance use to cope between sessions. |
| Resistance to opposite action at first. | Complete disengagement from skills for 2+ weeks. |
What to do if you recognize a red flag: Talk to your therapist or program coordinator directly. At Wellness Hills, your treatment team monitors these signals through weekly check-ins, diary card review, and clinical observation, but your own awareness matters. Recognizing a red flag early is not a sign of failure.
It is a sign that your current level of care may need to be adjusted, and that adjustment is a normal part of the treatment process. If you are experiencing suicidal thoughts at any point, call or text 988 immediately.
IOP, PHP, or Individual Therapy: Choosing the Right Level of Care for Depression
Choosing the right level of care depends on your daily functioning and symptom stability.
Individual DBT Therapy May Be Enough If…
- Depression is mild to moderate
- You’re functioning at work or school
- You can apply skills between sessions
- You have some support in place
IOP-Level DBT May Be the Right Fit If…
- Depression is affecting daily functioning
- Weekly therapy hasn’t been enough
- You need more consistency and accountability
At Wellness Hills, we offer two tracks:
- IOP 3 Evening: Meets Monday, Tuesday, and Thursday from 6–9 PM. This is ideal for those working or commuting in NJ during the day.
- IOP 5 Morning: Meets Monday through Friday from 9 AM–12 PM for those who need more daily structure.
Wellness Hills is located in Chester, NJ, in Morris County. Our evening IOP schedule is designed for adults commuting from surrounding areas, including Morristown, Hackettstown, Mendham, Parsippany, and the greater Morris, Hunterdon, and Somerset counties.
When Partial Hospitalization (PHP) is the Right Fit
- Depression is severe enough that daily clinical structure is needed to maintain safety and forward progress
- You’re having difficulty getting through the day without support
- You’re stepping down from a recent hospitalization or inpatient stay
Our PHP program (Mon–Sat) provides the highest level of outpatient structure for those stepping down from a hospital or avoiding inpatient care. If you are unsure which level of care is appropriate, the initial clinical evaluation is designed to determine that.
Depression Recovery Timeline: What Improves First and What Takes Longer
Setting realistic expectations helps prevent you from giving up too early.
Early Shifts (Weeks 2–4):
- Behavioral Activation: You might notice you are staying in bed less or following a basic routine.
- Awareness: You start to notice a dark spiral, as it happens, even if you can’t stop it yet.
- Language: You begin to name your feelings (like fear or shame) rather than just feeling a heavy, dark cloud.
Longer-Arc Changes (Months 2–4 and Beyond):
- Regulating your emotions even during high-stress moments at work or home.
- A decrease in the intensity and length of your depressive episodes.
- Healthier communication and boundaries in your relationships.
How Progress Is Measured in a DBT Program
In a structured DBT program, progress is not based on how you feel on any given day. It is tracked using standardized clinical tools and behavioral indicators.
Standardized assessments: Most evidence-based programs use tools such as the PHQ-9 (Patient Health Questionnaire-9) to measure depressive symptom severity at regular intervals, typically at intake, the program midpoint, and discharge.
The PHQ-9 scores depression on a 0-27 scale, where a reduction of 5 or more points is generally considered a clinically meaningful improvement. Your treatment team uses these scores, along with your self-report and clinical observations, to adjust your plan.
DBT diary cards: Between sessions, you track daily mood, urges, and skill use on a diary card. This is not busywork; it is a core component of the DBT model. Your therapist reviews the diary card at the start of each individual session to identify patterns, celebrate progress, and target the areas that are still stuck.
Over time, the diary card itself becomes evidence of change: fewer urges, more skill use, shorter depressive episodes.
Behavioral milestones: Clinical teams also track functional indicators that standardized tools may not fully capture: Are you attending sessions consistently? Are you completing homework? Are you re-engaging with activities you had previously dropped? Are interpersonal conflicts decreasing? These behavioral markers often shift before mood scores do, which is why giving up too early is one of the most common mistakes in depression treatment.
Typical program duration: IOP-level DBT programs typically run 8 to 12 weeks, with clinical reassessment at the midpoint to determine whether to continue, step down to a lower level of care, or adjust the treatment focus.
A full standard DBT curriculum (all four modules) generally takes 6 to 12 months when completed in an outpatient or IOP setting. At Wellness Hills, program length is individualized based on your progress, not a fixed calendar.
A Typical Week in Our DBT-Integrated IOP Program
Wellness Hills, located in Chester, New Jersey, designs its scheduling to fit the realities of local life. For many, our IOP for depression evening track provides the right balance.
- Monday Evening (6–9 PM): The week begins with group skills training focused on a specific module, such as emotion regulation. You will participate in a homework review from the prior week and a brief individual check-in.
- Mid-Week: Between sessions, the focus shifts to real-world application. It may involve using a DBT diary card to track your mood, urges, and the specific techniques you are practicing. This phase is critical for turning abstract concepts into functional habits.
- Thursday Evening (6–9 PM): The second group session of the week focuses on applying skills to real scenarios brought in by members. This is where you process the challenges of the week and refine your approach with peer support and clinical feedback.
You might work with a therapist like Abby Goodrich, LAC, to troubleshoott to troubleshoot why a specific skill feels difficult to use. Our psychiatric nurse practitioner, Paula Weisman, PMHNP-BC, is also available to help with medication management if that is part of your coordinated care plan.
Frequently Asked Questions About DBT for Depression
These are the questions we hear most often from people considering DBT during treatment for depression, particularly around how long it takes, whether medication is necessary, and what happens when life gets in the way of consistent attendance.
How long does DBT typically take to help with depression?
Most people see small shifts in their behavior within the first several weeks. However, completing a full DBT curriculum usually takes several months of consistent work.
Can DBT make depression worse before it gets better?
It can feel that way at first. Mindfulness practice may temporarily increase your awareness of painful emotions that you were previously avoiding or numbing. Opposite action may feel physically uncomfortable when you push against the urge to withdraw.
These are expected parts of the process, not signs that treatment is failing. If symptoms are worsening consistently (not just temporarily after a session), that is a clinical red flag your treatment team needs to know about. See the section above on red flags vs. normal discomfort.
What happens if I miss a DBT group session?
Consistency is a core part of how DBT works. Missing a session means missing skill instruction and peer practice that cannot be fully replicated in a makeup format. Most DBT programs, including ours, have attendance expectations built into the treatment agreement.
If life circumstances make attendance difficult, talk to your treatment team. It may indicate that a different schedule (such as our morning vs. evening IOP tracks) or a different level of care is a better fit.
Is DBT effective for depression without medication?
It can be, depending on severity. For mild to moderate depression, DBT skills training alone may be sufficient. For moderate to severe depression, particularly when it involves significant functional impairment, sleep disruption, or concentration problems, most clinical guidelines recommend combining skills-based therapy with psychiatric medication.
At Wellness Hills, medication is never required, but it is available and coordinated with your skills work when clinically appropriate.
How is DBT different from regular talk therapy?
Traditional talk therapy (psychodynamic or supportive counseling) is typically unstructured, insight-focused, and delivered in a one-on-one format. DBT is structured, skill-based, and delivered through a combination of individual therapy, group skills training, and between-session practice.
In traditional therapy, you might explore why you feel a certain way. In DBT, you also learn a specific technique for what to do about it, and you practice that technique until it becomes a default response.
Does insurance cover DBT programs in New Jersey?
Coverage for DBT-based IOP or PHP varies by plan, network status, authorization requirements, and medical-necessity criteria. Insurance benefits should always be verified before admission. At Wellness Hills, our admissions team can review your benefits and explain what your plan may cover before treatment begins.
Start With a Clinical Assessment
If depression is still showing up as shutdown, avoidance, emotional spirals, or difficulty following through day to day, a clinical assessment can determine whether a structured DBT-integrated program is the right next step.
At Wellness Hills in Chester, NJ, the process starts with a phone call. Our admissions team will verify your insurance coverage, answer your questions about scheduling (including our evening and morning IOP tracks), and connect you with our clinical team for an evaluation.
Call 973-532-5139 or schedule an assessment online to get started. Wellness Hills Mental Health is licensed by the New Jersey Department of Health (License #70290104).
If you are in crisis or experiencing thoughts of suicide, call or text 988 for immediate support.
Sources:
Mapping Dialectical Behavior Therapy Skills to Clinical Domains Implicated in Contemporary Addiction Research | PubMed Central (PMC) – A conceptual review explaining how DBT skills map to clinical domains such as negative emotionality, executive functioning, and quality of life, which is useful for supporting broader explanations of how DBT skills are applied in treatment.
Knowledge Center | Behavioral Tech Institute – A curated DBT resource hub from Behavioral Tech Institute with foundational information on DBT, including basics, implementation, and educational resources for clinicians, clients, and families.
DBT-Informed Treatment in a Partial Hospital and Intensive Outpatient Program: The Role of Step-Down Care | PubMed Central (PMC) – A study examining DBT-informed PHP and IOP treatment, including step-down care, that found significant reductions in depression, anxiety, hopelessness, and overall suffering from intake to discharge.
Editorial Standards
Our Editorial Policy
Our editorial standards keep our mental health content accurate, compassionate, and evidence-informed. Articles are developed using credible sources, reviewed for medical accuracy when needed, and regularly updated.