If you are searching for evidence-based therapy for depression in NJ, you are likely looking for more than just a place to talk. When depression deepens, it stops being about having a bad week and starts being about a collapse in daily functioning. The goal of high-quality treatment is to move beyond simple insight and into measurable recovery.
At Wellness Hills, we view proven depression treatments as a matching process. The best therapy for depression isn’t a single universal brand; depression treatment is built around three decisions: which therapy approach fits the presentation, which level of care fits the current level of impairment, and how progress will be measured and reviewed. That is what evidence-based depression therapy looks like in practice.
On this page, we explain how CBT, Behavioral Activation, DBT-informed treatment, ACT, and level-of-care planning may be used in depression treatment; when outpatient therapy may be enough, when a more structured program may be clinically appropriate, and how treatment response is monitored over time. For a broader overview of depression, its causes, and how it’s diagnosed, visit our depression overview page.
When Depression Stops Responding to Insight Alone
Many people do not arrive at treatment saying, “I have major depressive disorder.” They arrive saying they feel flat, exhausted, shut down, detached, or unlike themselves. Distinguishing sadness, burnout, and clinically significant depression matters because the right treatment depends on whether the problem is temporary emotional pain, stress-related depletion, or a depressive condition that is affecting motivation, functioning, and day-to-day life.
The Difference Between Sadness, Burnout, and Clinically Significant Depression
While sadness, burnout, and depression can all involve a low mood, they affect a person in very different ways, especially in how they influence energy, motivation, and thinking.
Time-Limited Sadness: A Temporary Emotional Response
Sadness is a normal reaction to loss or difficult experiences. It usually comes and goes in waves.
Key Sign: The person can still enjoy small moments. Someone sad may still laugh, feel distracted for a while, or enjoy time with others. Their self-esteem usually stays intact, and they do not experience the strong mental or physical slowing seen in major depression.
Burnout: Stress-Related Exhaustion
Burnout happens when a person feels drained after long periods of stress, often related to work or caregiving.
Key Sign: The symptoms are tied to a specific situation. For example, someone may feel exhausted and frustrated at work but feel more like themselves during time off.
Main Difference: The person’s energy is depleted, but their ability to enjoy life may remain. If the stress is reduced or they get proper rest, their motivation and personality usually return.
Major Depressive Disorder: A Deeper Mental Health Condition
Major Depressive Disorder (MDD) affects how the brain processes emotions, motivation, and daily functioning. Doctors often look for several key signs.
Loss of Pleasure (Anhedonia): This is more than feeling sad. The person may lose the ability to feel any enjoyment. Activities that used to feel rewarding may feel empty or flat.
Changes in Movement and Energy: Some people move and speak more slowly and feel physically heavy. Others may feel restless, pace, or unable to relax, even though they feel exhausted.
Thinking and Concentration Problems: Depression can make it hard to focus, make decisions, or organize thoughts. Even simple choices like deciding what to eat can feel overwhelming.
When depression is driving avoidance, loss of routine, indecision, and reduced functioning, insight alone is often not enough. At that point, treatment usually needs to focus on behavior change, symptom tracking, and the right level of structure, not just self-understanding. If you’re unsure whether what you’re experiencing is clinical depression, a PHQ-9 screening can help you see where your symptoms fall.
Why Depression Often Involves Avoidance, Rumination, and Loss of Functioning
Depression often creates a self-reinforcing cycle. Rumination can lead to withdrawal. Withdrawal can reduce structure, activity, and social contact. As routine breaks down, symptoms often deepen. In treatment, these patterns are addressed as clinical targets rather than character flaws. The goal is to interrupt the cycle through structured therapy, behavioral change, and ongoing review of whether functioning is improving.
When Weekly Outpatient Therapy May Not Be Enough for the Current Level of Impairment
Weekly outpatient therapy can be effective for many people with depression, especially when functioning is mostly intact. But when depression is causing significant withdrawal, poor self-care, worsening work or school performance, persistent hopelessness, or reduced ability to manage daily responsibilities, once-weekly therapy may not provide enough structure or support. In those cases, clinicians may consider whether a more intensive level of care is appropriate.
How the Wellness Hills Clinical Team Selects CBT, Behavioral Activation, DBT, or ACT for Your Depression
Our clinical team, led by Program Director Leigh Rasmussen, LPC, LCADC, selects from CBT, Behavioral Activation, DBT, and ACT based on the specific pattern of symptoms, functioning, and treatment history identified in the intake assessment.

CBT for Negative Thought Patterns, Hopelessness, and Self-Defeating Beliefs
Cognitive Behavioral Therapy (CBT) is often used when depression is maintained by automatic negative thoughts, rigid self-judgments, hopeless predictions, or distorted interpretations of everyday events.
Treatment focuses on identifying these patterns, testing them against reality, and building more accurate and workable thinking. At Wellness Hills, CBT is delivered in individual sessions, using structured thought records and between-session skill assignments that are reviewed at each appointment.
Behavioral Activation for Shutdown, Isolation, Anhedonia, and Loss of Routine
Behavioral Activation is sometimes described as a component of CBT, but it is increasingly recognized as a powerful therapy approach in its own right. Behavioral Activation focuses on the reality that depression often shrinks a person’s life. Activities disappear.
Social contact fades. Motivation declines. The treatment goal is often to reverse this cycle by helping the person rebuild meaningful activity patterns step by step.
For individuals experiencing severe anhedonia or inactivity, Behavioral Activation may become a central component of effective therapy for depression. Clinicians use activity scheduling with explicit pleasure and mastery ratings so progress is tracked numerically, not subjectively.
DBT-Informed Treatment for Dysregulation, Self-Harm Urges, and Crisis-Driven Patterns
When depression includes intense emotional swings, self-harm urges, or difficulty staying regulated under stress, DBT-informed treatment may be appropriate. In those cases, therapy may focus more heavily on distress tolerance, emotion regulation, and crisis-management skills so treatment can stabilize before deeper work continues. DBT skills are introduced in both individual and group formats; the group component is available within the IOP track.
ACT for Rumination, Cognitive Fusion, and Getting Stuck in Depressive Thinking
Acceptance and Commitment Therapy (ACT) may be helpful when depression is driven by a persistent mental struggle with thoughts and feelings. Instead of trying to eliminate every painful thought, treatment helps the person reduce entanglement with those thoughts, reconnect with values, and take workable action even while symptoms persist. ACT work at Wellness Hills often involves values-clarification exercises completed between sessions to anchor behavioral commitments.
Depressive Presentations That Change the Therapy Plan
Depression treatment planning changes when the presentation includes anxiety, trauma symptoms, obsessive-compulsive features, suicidality, severe functional decline, or possible bipolar features. These are not side notes. They directly affect which therapy strategies are used, whether a psychiatric review is needed, and whether outpatient therapy is enough.

Major Depressive Disorder With Anxious Distress
Many people experiencing Major Depressive Disorder also experience significant anxiety symptoms. When anxious distress is present, clinicians often track symptoms using tools like the GAD-7 and incorporate anxiety-focused skills into therapy.
Persistent Depressive Disorder and Long-Term Low Motivation
According to the National Center for Biotechnology Information, Persistent Depressive Disorder (PDD) is defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as a condition that combines the earlier diagnoses of dysthymic disorder and chronic major depressive disorder.
PDD is a type of long-lasting depression that usually continues for two years or more. It may not always feel as intense as a major crisis, but it can still be draining because the symptoms continue for a long time.
Because the symptoms develop slowly, many people start to think that low motivation or low energy is just part of their personality. Treatment often focuses on steady, gradual progress, while carefully tracking changes in how a person functions in daily life.
Depression With Trauma Features, Panic, or OCD Traits
Depression can also overlap with trauma symptoms, panic attacks, or obsessive-compulsive patterns. In these cases, the treatment plan may need to incorporate trauma-focused therapy, exposure-based work, or specialized anxiety interventions.
Depression With Suicidality or Severe Functional Decline
When depression includes suicidal thinking, severe self-neglect, or significant functional collapse, clinicians may recommend a more structured level of care.
Risk assessment tools such as the Columbia Suicide Severity Rating Scale can help clinicians evaluate safety and determine appropriate treatment planning.
Depression With Bipolar Features or Medication Complexity
Some individuals who initially present with depression may later show signs of bipolar mood patterns or complex medication histories.
In these cases, psychiatric evaluation and medication management often become a more central component of treatment.
What Proven Depression Treatment Looks Like Across OP, IOP, and PHP
The same therapy model is not delivered at the same intensity in every setting. A key part of evidence-based depression treatment is determining how much structure, frequency, and clinical monitoring a person needs right now.
At Wellness Hills, level-of-care decisions are based on severity, functioning, safety, treatment history, and the amount of support needed between sessions.
| Level of Care | Frequency | Clinical Focus |
|---|---|---|
| Outpatient (OP) | 1–2 sessions/week | Maintenance, mild-to-moderate symptom management. |
| Intensive Outpatient (IOP) | 3–5 days/week | Structured skill-building for moderate functional impairment. |
| Partial Hospitalization (PHP) | Daily (6 days/week) | High-acuity support: a bridge for those at risk of inpatient hospitalization. |
The purpose of this framework is not to push everyone into the highest level of care. It is to avoid both under-treatment and over-treatment by matching structure to current clinical need.
When Outpatient Therapy Is Clinically Appropriate
Outpatient therapy remains a legitimate and effective level of care for many individuals.
People who maintain stable functioning at work, in school, or in family life may benefit from weekly therapy combined with skill development and symptom monitoring.
When IOP Offers the Structure that Weekly Therapy Cannot
An Intensive Outpatient Program can provide several therapy sessions per week, often including both individual and group therapy.
For individuals whose depression is interfering with work performance, relationships, or daily functioning, this additional structure can make treatment more effective than weekly sessions alone.
When PHP Is Used for Depression That Is Affecting Daily Functioning
A Partial Hospitalization Program offers a higher level of structure while still allowing individuals to live at home. PHP typically involves full-day treatment schedules with multiple therapeutic interventions and psychiatric oversight.
How Step-Up and Step-Down Decisions Are Made
Level of care is reviewed over time, not chosen once and left unchanged. If symptoms worsen, functioning drops, safety concerns increase, or weekly care is no longer enough, clinicians may recommend stepping up to a more structured setting. As stability improves, treatment can be stepped down so support remains appropriate without becoming excessive.
Measurement-Based Depression Care Using PHQ-9, GAD-7, and Functional Tracking
A treatment plan should not be judged by attendance alone. Evidence-based depression treatment includes ongoing review of whether symptoms are changing, whether functioning is improving, and whether the current level of care still fits.
Tools such as the PHQ-9, GAD-7, and suicide-risk screening can support that process, but they are used alongside clinical judgment and day-to-day functioning.
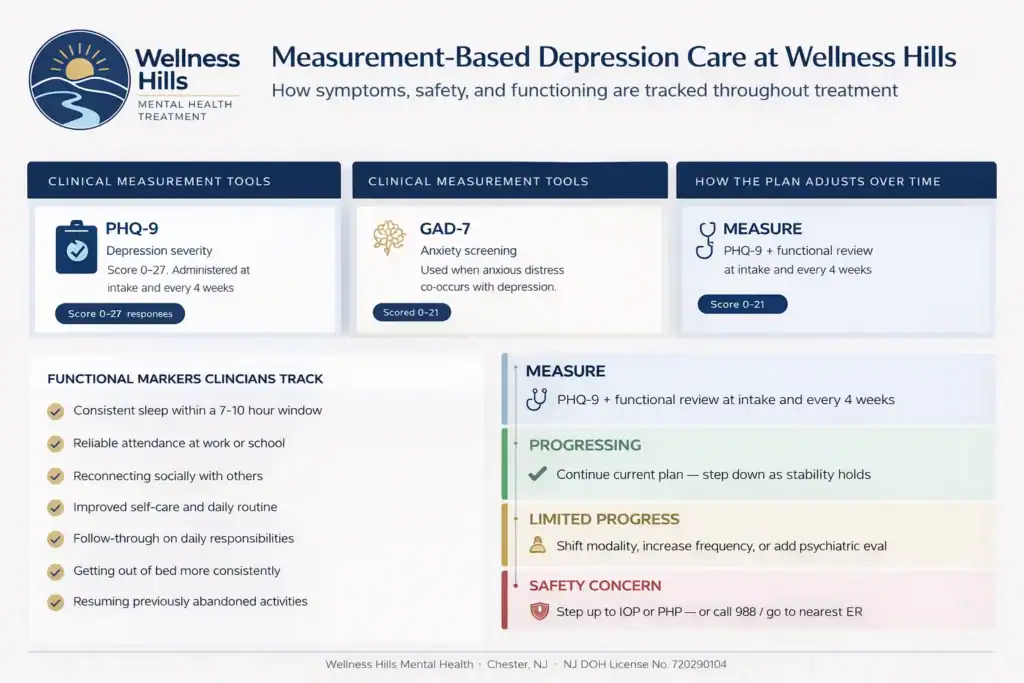
Why Symptom Scores Are Only Part of the Picture
Depression severity scales can help track change over time, but a score by itself does not tell the full story. Clinicians also look at whether the person is getting out of bed more consistently, attending work or school more reliably, reconnecting socially, improving self-care, sleeping more regularly, and showing better follow-through with daily responsibilities.
How Safety and Treatment Response Are Monitored
If someone is feeling extremely overwhelmed or hopeless, doctors use a tool called the Columbia Suicide Severity Rating Scale to check for suicide risk. They don’t rely only on the score. They also consider a person’s behavior, stress levels, and coping abilities to ensure the right support is in place.
An evidence-based therapy program for depression provides structured treatment, but it is not meant for suicide emergencies. If any of the following are happening, you should seek immediate help instead of starting the program:
- You are having active thoughts of suicide or have a plan to harm yourself
- You feel unable to keep yourself safe
- You are in a serious mental health crisis that needs immediate care
In these situations, call 911, go to the nearest emergency room, or contact 988 for crisis support. Once you are safe and stable, the clinical team can help determine the appropriate next step in your treatment.
How the Treatment Plan May Change Over Time
Treatment should change when the clinical picture changes. If a person is not improving, clinicians may shift the therapeutic focus, increase structure, recommend a higher level of care, or add psychiatric evaluation when clinically indicated. If symptoms and functioning improve, treatment can be stepped down so support remains appropriate to current need.
Therapy Alone vs Therapy Plus Medication for Depression
One treatment-planning question in depression care is whether psychotherapy alone is a reasonable starting point or whether psychiatric evaluation should also be considered. The answer depends on symptom severity, recurrence, vegetative symptoms, safety concerns, treatment history, and how much impairment is present.
Medication evaluation and management at Wellness Hills is provided by Paula Weisman, PMHNP-BC, a Psychiatric Nurse Practitioner, who collaborates directly with the therapy team on integrated treatment planning.
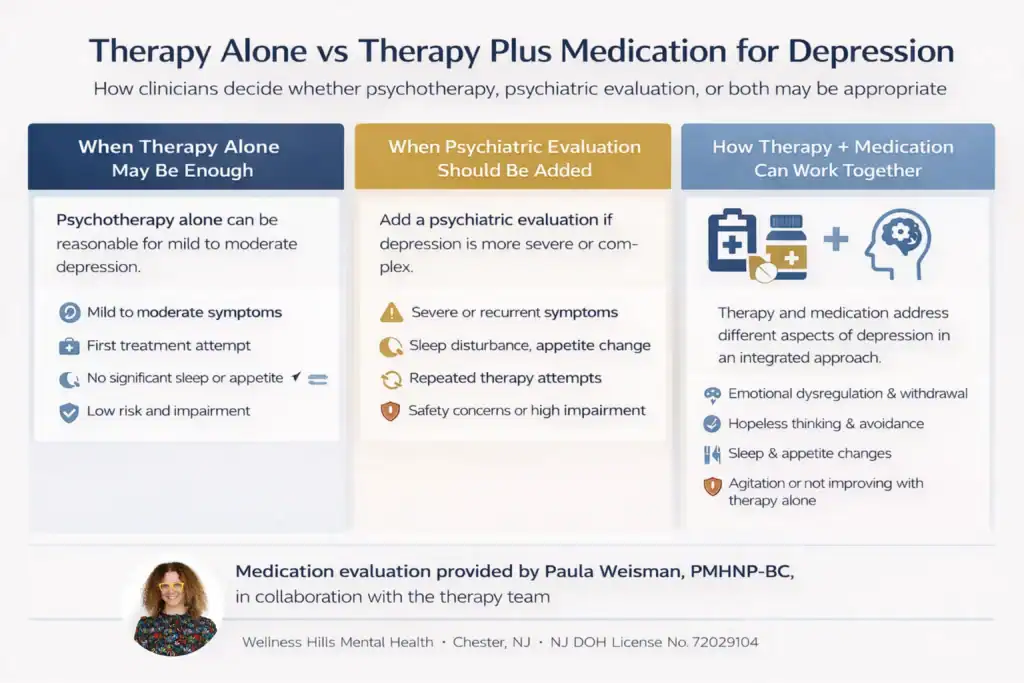
When Psychotherapy May Be Enough
For mild to moderate depression, psychotherapy alone may be a reasonable starting point. Many people experience meaningful improvement through structured therapy interventions.
When Psychiatric Evaluation Should Be Added
For more severe depression, recurrent episodes, or significant neurovegetative symptoms such as sleep disruption or appetite changes, a psychiatric evaluation may be appropriate.
Medication management may be provided by clinicians, such as Psychiatric Nurse Practitioners, who work collaboratively with therapists.
How Psychotherapy and Medication May Work Together
Therapy and medication serve different functions. Psychotherapy targets patterns such as hopeless thinking, avoidance, withdrawal, emotional dysregulation, and impaired coping. Medication may be considered when symptom severity, recurrence, sleep disruption, appetite change, agitation, or limited response to therapy alone suggest that psychiatric support should be evaluated as part of the plan.
Insurance, Clinical Fit, and What to Expect Before Starting Depression Treatment in New Jersey
Before treatment begins, the clinical and admissions teams work to clarify two questions: what level of care is clinically appropriate and what the insurance plan is likely to authorize. Those are related, but they are not identical.
The goal is to align care with clinical need while also reviewing practical coverage details before treatment begins. Wellness Hills accepts Aetna, Cigna, BCBS NJ, UnitedHealthcare, Horizon, etc. Call 973-532-5139 or use our online insurance verification form to confirm your specific benefits before your first appointment.

What Insurance Reviews for Medical Necessity
Insurance companies review your medical records to ensure your treatment is medically necessary. They want to ensure that the care you are receiving is the right fit for your needs and adheres to standard medical practice.
For more serious programs, like staying at a treatment center or going to an all-day clinic, insurance companies often look for proof of two main things:
- Safety: Can you stay safe at home, or do you need 24/7 support?
- Effectiveness: Would a simpler treatment (like seeing a therapist once a week) actually work, or do you need something more intense to get better?
Coverage for higher levels of care usually depends on whether the documentation shows that the service is medically necessary based on symptom severity, safety, functional impairment, and the likelihood that a lower level of care would be insufficient.
What a Depression Assessment Should Clarify
A comprehensive assessment typically evaluates:
- Diagnosis and symptom pattern
- Co-occurring conditions
- Suicide risk
- Treatment history
- Current functioning
- Treatment goals
This information helps clinicians determine which therapy types for depression and level of care may be appropriate.
Which Licensed Professionals May Be Involved in Care
Depression treatment may involve multiple licensed professionals depending on the level of care and the needs of the individual. This can include licensed professional counselors, licensed clinical social workers, psychologists, and psychiatric nurse practitioners when medication evaluation or medication management is clinically appropriate.
Clinical care at Wellness Hills treatment is delivered by a multidisciplinary team including Leigh Rasmussen, LPC, LCADC, and fully licensed clinicians. The facility is licensed by the NJ Department of Health (License No. 70290104) and accredited by the Joint Commission.
What Depression Treatment at Wellness Hills Looks Like in Practice
Evidence-based care is not defined solely by the names of therapies used. It is also defined by how the treatment plan is built, reviewed, and adjusted over time. At Wellness Hills Mental Health Treatment in Chester, New Jersey, depression treatment begins with assessment, continues with modality and level-of-care matching, and is reviewed against both symptom change and day-to-day functioning.
During the assessment process, clinicians look at symptom pattern, severity, safety, treatment history, co-occurring conditions, and current functioning. That information helps determine whether weekly outpatient therapy is appropriate or whether a more structured setting should be considered.
Once treatment begins, progress is reviewed using symptom measures, clinical observation, and changes in real-life functioning. If the current approach is not sufficiently effective, the plan may be adjusted by shifting therapeutic focus, increasing structure, or adding a psychiatric evaluation when clinically appropriate.
What to Expect During Your First 30 Days of Depression Treatment at Wellness Hills
Week 1 (Clinical Assessment and Level-of-Care Matching): A licensed clinician conducts a 60–90-minute intake assessment covering your symptoms, functioning, safety, and treatment history, using the PHQ-9 and GAD-7. By the end of Week 1, your therapy modality and level of care, outpatient, IOP, or PHP, are selected based on that data, not assumption.
Weeks 2–4 (Therapy Modality Introduction and Initial Skill Building): Active treatment begins with structured skill introduction, thought records for CBT, activity scheduling for Behavioral Activation, distress tolerance for DBT, or values-clarification for ACT, with between-session assignments reviewed at every appointment. Your first PHQ-9 progress review occurs at the end of Week 4, where a 5-point reduction is the benchmark for a meaningful initial response.
Weeks 5–8 (Progress Review and Plan Adjustment): If Week 4 showed limited progress, the clinical team formally reviews whether the modality, structure, or level of care needs to change; this is a clinical recalibration, not a setback. Relapse prevention planning also begins here, regardless of how well treatment is going.
Discharge and Step-Down (Continuing Care Planning): Completing IOP or PHP at Wellness Hills concludes with a written continuing care plan that covers your outpatient follow-up schedule, personal warning signs, and a crisis plan. If symptoms return after step-down, re-entry into structured care is available without a full new intake.
Frequently Asked Questions About Evidence-Based Treatment for Depression
The questions below address the most common decision points patients and families raise before starting depression treatment at Wellness Hills, including how therapy modalities are selected, when a more structured level of care is appropriate, and what role medication plays in the overall plan.
Can therapy work for depression without medication?
In some cases, yes. In others, psychiatric evaluation may be appropriate based on severity, recurrence, vegetative symptoms, safety concerns, or limited response to therapy alone.
Is progress measured during depression treatment?
Yes. Good depression treatment should involve more than attending sessions. Clinicians may use symptom scales, suicide-risk screening when needed, and review of real-life functioning to determine whether the treatment plan is helping.
How do clinicians decide which therapy approach to use for depression?
The treatment approach depends on the symptom pattern. For example, clinicians may emphasize CBT when negative thought patterns are driving hopelessness, Behavioral Activation when depression is causing shutdown and withdrawal, DBT-informed work when dysregulation or self-harm urges are present, and ACT when rumination or cognitive fusion is keeping the depression in place.
How do you know whether weekly therapy is enough for depression?
Weekly outpatient therapy may be appropriate when functioning is mostly intact, and symptoms can be managed safely in that setting. When depression is causing significant withdrawal, poor self-care, worsening performance at work or school, or rising safety concerns, a more structured level of care may need to be considered.
Start With a Confidential Depression Assessment
If you are looking for evidence-based therapy for depression in New Jersey and are unsure whether weekly therapy, IOP, or PHP is the right fit, the next step is a confidential assessment. That process helps clarify symptom pattern, current functioning, safety needs, and whether psychiatric evaluation should also be considered. You can verify your insurance or speak with our team in Chester, NJ, at 973-532-5139.
Sources:
Persistent Depressive Disorder – StatPearls – NCBI Bookshelf – Reviews persistent depressive disorder, including diagnostic criteria, clinical presentation, risk factors, functional impairment, and treatment considerations.
Columbia-Suicide Severity Rating Scale (C-SSRS) | Columbia University Department of Psychiatry – Explains the C-SSRS suicide risk assessment tool, including how it helps identify suicidal ideation, behavior, risk severity, and immediacy of support needs.
National 911 Program | 911.gov – Official federal resource stating that if someone is experiencing an emergency, they should call 911 immediately.
Mental Health Prior Authorization (PA) Guidance and Medical Necessity Training | New Jersey Human Services (PDF) – NJ FamilyCare Behavioral Health Integration training covering mental health prior authorization, clinical documentation, and medical necessity review for behavioral health services.
Editorial Standards
Our Editorial Policy
Our editorial standards keep our mental health content accurate, compassionate, and evidence-informed. Articles are developed using credible sources, reviewed for medical accuracy when needed, and regularly updated.