Most people who type this question into a search bar aren’t asking because they’re fine. They’re asking because something has been getting worse, or quieter, or smaller than it used to be, and they want to know if what they’re feeling counts as a real problem. The signs you need professional help for anxiety aren’t always dramatic.
What follows is a guide to recognizing whether you’ve crossed a threshold worth taking seriously, why people wait longer than they should, and what professional help actually looks like, because it’s rarely a binary choice between fine on your own and in a hospital. This is informational, not a substitute for clinical evaluation.
Quick Answer: When Anxiety Needs Professional Help
- Anxiety crosses a clinical threshold when it persists most days for weeks, disrupts functioning, or feels disproportionate.
- Professional help is valuable before a crisis hits; you don’t need to wait until symptoms become severe.
- Racing heart, GI issues, sleep disruption, muscle tension, and growing avoidance are common threshold markers.
- Treatment ranges from weekly therapy to intensive outpatient (IOP) and partial hospitalization (PHP), matched to severity.
- Suicidal thoughts, panic that won’t subside, or inability to self-care: call 988, the emergency department, or 911.
The Quiet Reasons People Wait Too Long
Most people who eventually get help for anxiety say they wish they’d done it sooner. What kept them from acting wasn’t a lack of symptoms; it was a specific set of cognitive moves that made their experience feel less serious than it was.
If you’re asking whether you should see a therapist for anxiety, you’re probably already past the threshold where the question is worth taking seriously. Among clients who eventually enroll in our program, the most common reason for delaying enrollment is some variation of “I should be able to handle this on my own.”
- “It’s just stress.” Stress is event-driven and resolves when the event does. Anxiety persists past the trigger, or generalizes from one worry to many.
- “Everyone feels this way.” Some worry is universal. The criterion isn’t whether other people experience anxiety; it’s whether yours is interfering with how you actually live.
- “I should be able to handle this on my own.” Self-management works for sub-clinical anxiety. Clinical-level anxiety responds to evidence-based treatment; willpower isn’t a substitute for the right approach.
- “It comes and goes, so it’s not that bad.” Episodic anxiety can still be clinically significant, especially when episodes are intensifying or spreading to new contexts.
- “I’m still functioning, so I must be fine.” Functioning while exhausted, dreading mornings, or running on adrenaline isn’t the same as being well.
What Crossing the Line Actually Looks Like
Clinicians don’t judge anxiety by one bad day. They look at six dimensions over time: duration (how long), frequency (how often), control (how hard the worry is to interrupt), functional impairment (work, sleep, relationships, daily responsibilities), avoidance (how much your life is organized around what you don’t do), and safety or medical concern. The most reliable threshold signals show up in pattern, function, and physiology, not in any single moment of intensity.
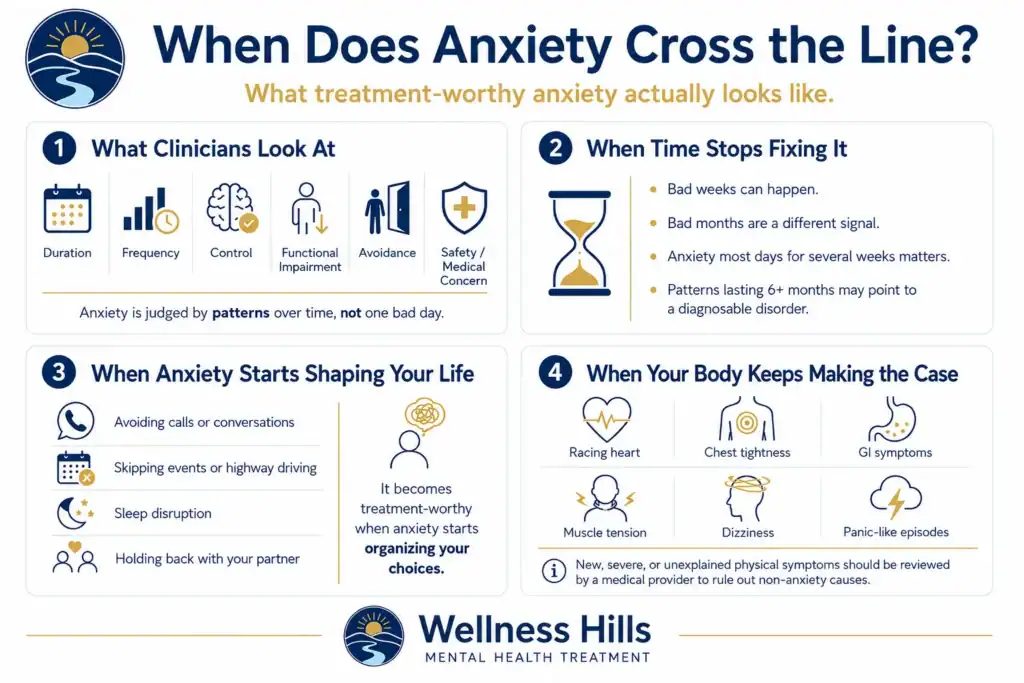
When Time Stops Fixing It
Bad weeks happen to everyone. Bad weeks that turn into bad months are a different category. Anxiety lasting most days for several weeks is a meaningful signal; patterns running six months or more often indicate something diagnosable, like generalized anxiety disorder. The clearest version of this isn’t dramatic; it’s the slow realization that you can’t remember when you last felt like yourself.
When Anxiety Starts Shaping Your Life Instead of Just Visiting It
Watch for the choices you’re quietly making to accommodate it: not taking the call, not driving on the highway, not going to the event, not sleeping through the night, not bringing things up with your partner. Anxiety becomes treatment-worthy when it stops being something that happens to you and starts being something that organizes you.
When Your Body Keeps Making the Case
Persistent racing heart, chest tightness, GI symptoms, muscle tension, dizziness, panic-like episodes. Bodies often register anxiety before minds admit to it. A medical provider should review new, severe, or unexplained physical symptoms to rule out non-anxiety causes such as cardiac, thyroid, or vestibular conditions. These markers don’t replace a clinical evaluation; they help you decide whether to schedule one.
When Your Coping Starts Working Against You
Anxiety doesn’t just create symptoms; it creates coping behaviors. Some quietly make it worse over time, even when they offer real short-term relief. Signs you need therapy for anxiety often show up not in the anxiety itself but in the workarounds you’ve built. Recognizing the pattern is often when people decide to ask for help.
- Avoidance: Skipping things you used to do, meetings, drives, calls, errands, and plans. The relief is real, and so is what it costs you. Avoidance is usually what makes anxiety progressive.
- Reassurance-seeking and compulsive checking: Googling symptoms for hours, asking your partner whether something looks okay over and over, re-reading emails, checking locks until the worry briefly settles, then needing to check again.
- Substances, food, work, or numbing: When alcohol, weed, screens, food, or overwork become the main way you take the edge off, you’ve added a second problem on top of the first.
- Isolation that stopped being recovery: What started as needing space to recharge became how you live, fewer plans, fewer texts answered, fewer people who know how you’re doing.
Anxiety Isn’t One Disorder
The threshold signals in this article apply broadly across anxiety disorders, but specific patterns may point to different diagnoses. Generalized anxiety disorder (GAD), social anxiety disorder, panic disorder, specific phobias, and agoraphobia each have characteristic features.
Related conditions like OCD (intrusive thoughts paired with compulsions) and PTSD (intrusive re-experiencing and hyperarousal) can present with anxiety symptoms but typically require distinct treatment approaches.
What Kind of Professional Help Fits Your Anxiety Symptoms?
Most people picture getting help as weekly therapy. For some, that’s exactly right. For others, weekly therapy isn’t enough, and the gap between an hour a week and inpatient hospitalization is where most anxiety treatment actually happens. Knowing when to get help for anxiety is one question; knowing what level fits where you actually are is a different one.
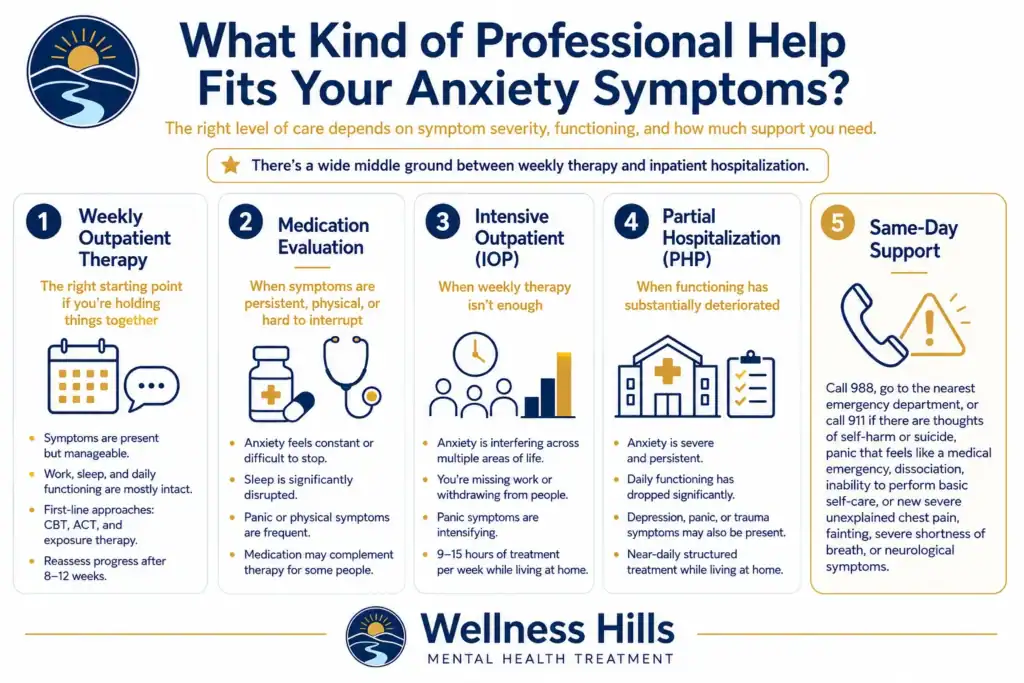
Weekly Outpatient Therapy - The Right Starting Point If You're Holding Things Together
Symptoms are present and disruptive, but you’re maintaining work, sleep, and basic functioning. You can engage with what you learn between sessions and apply it to daily life.
Evidence-based outpatient approaches include Cognitive Behavioral Therapy (CBT), which targets anxious predictions, catastrophic thinking, and the avoidance and safety behaviors that maintain anxiety; Acceptance and Commitment Therapy (ACT), which builds a different relationship to anxious thoughts while moving toward valued action; and exposure therapy, which gradually returns people to avoided situations rather than organizing life around them.
Per APA practice guidelines, these are first-line interventions for most anxiety disorders, with response typically reassessed at 8-12 weeks.
Medication Evaluation - When Symptoms Are Persistent, Physical, or Hard to Interrupt
A medication evaluation may be appropriate when anxiety is persistent, sleep is significantly disrupted, panic symptoms are frequent, or physical symptoms are making daily functioning difficult.
Psychiatrists and psychiatric nurse practitioners assess whether medication may help, whether symptoms could overlap with another condition, and how medication would fit alongside therapy.
Medication is not the right choice for everyone, and therapy alone is sufficient for many people. For others, therapy and medication together provide better support than either alone.
Intensive Outpatient (IOP) - When Weekly Isn't Enough
Anxiety is interfering across multiple domains. You’ve tried outpatient therapy and need more structure than one session a week provides. You’re missing work, withdrawing from people, or experiencing intensifying panic attacks. IOP for anxiety offers nine to fifteen hours of structured treatment per week while you keep living at home.
Partial Hospitalization (PHP) - When Functioning Has Substantially Deteriorated
Anxiety is severe and persistent. Daily functioning has dropped significantly. Co-occurring depression, panic disorder, or trauma symptoms are present. PHP provides near-daily structured treatment while you still live at home, the highest level of outpatient care.
Crisis and Same-Day Support
Thoughts of self-harm or suicide, panic episodes that aren’t responding to grounding, and feel indistinguishable from a medical emergency, dissociation, or inability to perform basic self-care. Call 988 (the Suicide and Crisis Lifeline), go to your nearest emergency department, or call 911. After acute stabilization, structured outpatient care often becomes the right next step.
Because anxiety can mimic medical conditions, seek urgent medical evaluation for new, severe, or unexplained chest pain, fainting, severe shortness of breath, or neurological symptoms, as these may indicate non-anxiety causes that require medical workup.
One Question Worth Sitting With
Some of the uncertainty is part of the process; a clinical assessment is designed in part to answer the “is this bad enough?” question for you. If you want one framework to clarify where you are, sit with this question:
Is anxiety only something I feel, or is it changing how I live?
- If it’s uncomfortable but not changing your behavior, weekly therapy or self-guided coping may be enough.
- If it’s shaping your sleep, work, relationships, avoidance patterns, or daily decisions, a professional evaluation is reasonable.
- If safety concerns, escalating substance use, or major functional impairment are present, don’t wait.
If the answer is “I’m not sure,” that uncertainty is itself a valid reason to request an assessment. You don’t need to know the right level of care before reaching out. The point of the first conversation is to clarify what’s happening, what risks are present, and what kind of support fits.
Frequently Asked Questions
A few practical questions tend to remain once the framework above has been worked through. The answers below address the most common questions: when to act, who to see, how long to continue a course of treatment, and what to do when daily life is affected in ways the body and mind can’t fully explain.
When is anxiety too much to handle on your own?
Anxiety may be too much when it lasts most days for several weeks, interferes with work, sleep, relationships, or daily functioning, or feels disproportionate to its triggers. You don’t have to wait until it’s severe to consult a mental health professional; earlier intervention generally produces better outcomes.
Should I see a therapist or a psychiatrist for anxiety?
Therapists deliver talk-based treatment like CBT, exposure therapy, and ACT. Psychiatrists and psychiatric nurse practitioners evaluate whether medication is appropriate. Many people benefit from both, and coordinated programs offer both under one roof.
How long should I wait before getting help for anxiety?
If anxiety symptoms have lasted more than a few weeks and are interfering with a major area of your life, there’s no benefit to waiting. Many people delay seeking help for months or years and later wish they hadn’t.
What if weekly therapy hasn't been enough?
If anxiety hasn’t improved after a consistent trial of outpatient therapy, options include reassessing the approach, adding medication support, or stepping up to a higher level of care such as an Intensive Outpatient Program.
Can anxiety cause physical symptoms every day?
Yes. Anxiety commonly produces daily physical symptoms, including muscle tension, GI issues, racing heart, sweating, dizziness, restlessness, and sleep disruption. That said, new, severe, or unexplained physical symptoms, especially chest pain, fainting, shortness of breath, or neurological symptoms, should be reviewed by a medical provider to exclude non-anxiety causes such as cardiac, thyroid, or vestibular conditions.
Can I get help for anxiety without medication?
Yes. Many people are treated effectively with therapy alone. CBT, ACT, and exposure-based approaches are considered first-line interventions for most anxiety disorders. A medication evaluation may be appropriate when symptoms are persistent, severe, physical, or not improving with therapy alone, but medication is not required and isn’t the right choice for everyone. The decision typically reflects severity, individual preference, prior treatment response, and clinician input.
If You're in New Jersey
Many New Jersey adults delay treatment because they’re trying to keep up with work, commutes, caregiving, or school. Starting doesn’t require leaving home or entering inpatient care.
A typical first step is a confidential assessment, not a commitment to treatment. Insurance verification can clarify coverage for outpatient therapy, medication management, IOP, and PHP, including deductibles, copays, and prior authorization, before any treatment decision is made. Wellness Hills’ anxiety treatment program in NJ serves adults across the state through outpatient, IOP, and PHP levels of care.
If safety concerns are present, call 988, go to the nearest emergency department, or call 911 before routine admissions. For broader statewide referrals or system navigation, NJ Mental Health Cares provides information and referral support across New Jersey.
Take the Next Step
If anxiety is affecting your sleep, work, relationships, or daily responsibilities. Wellness Hills can help you understand what level of support might be right for you. Our team can talk through your symptoms, schedule, and treatment options, including outpatient therapy, IOP, and PHP. No commitment to treatment is required to start the conversation.
Request an Anxiety Assessment: Verify Insurance | Talk With Admissions
Sources:
National Institute of Mental Health (NIMH) | Generalized Anxiety Disorder: What You Need to Know – Official NIMH resource explaining GAD symptoms, diagnostic considerations, co-occurring conditions, and treatment options, including psychotherapy, medication, or both.
Center for Addiction and Mental Health (CAMH) | Anxiety: Diagnosis – Clinical resource explaining how anxiety disorders are assessed, including distress, impairment, persistence, differential diagnosis, and the need to match symptoms to the appropriate anxiety disorder.
National Institute of Mental Health (NIMH) | Anxiety Disorders – NIMH overview of anxiety disorders, including common symptoms, types of anxiety disorders, risk factors, and treatment options.
American Psychological Association (APA) | Guidelines for Practitioners – APA resource for professional practice guidance related to psychological intervention and care.
Substance Abuse and Mental Health Services Administration (SAMHSA) | 988 Suicide & Crisis Lifeline – Federal resource explaining 988 as a national crisis support service offering 24/7 judgment-free support for mental health, substance use, and related crises by call, text, or chat.
NJ Mental Health Cares | New Jersey Behavioral Health Information and Referral Service – New Jersey resource that connects residents with behavioral health information, referral support, supportive counseling, psychoeducation, advocacy, and help finding services such as inpatient, outpatient, housing, legal, employment, rehabilitation, and self-help resources.
Editorial Standards
Our Editorial Policy
Our editorial standards keep our mental health content accurate, compassionate, and evidence-informed. Articles are developed using credible sources, reviewed for medical accuracy when needed, and regularly updated.