Cognitive behavioral therapy for anxiety has strong research support; it’s one of the most extensively studied psychotherapies for anxiety disorders and a first-line recommendation in clinical guidelines.
Most people searching for CBT for anxiety aren’t looking for a definition. They want to know whether it’ll work for their specific anxiety, what sessions actually involve, and whether weekly therapy will be enough.
This guide covers what CBT targets across anxiety subtypes, what a session looks like, what improves first, the core techniques, and when weekly outpatient is enough and when it isn’t, alongside broader anxiety treatment considerations.
Quick Answer
- CBT is a structured, time-limited therapy targeting the thoughts and avoidance patterns that keep anxiety active.
- Strong evidence for GAD, panic disorder, social anxiety, health anxiety, and specific phobias (OCD requires the ERP variant; PTSD calls for trauma-focused CBT or CPT).
- Typical course: 12-20 weekly sessions in outpatient, faster pace in IOP or PHP.
- Not thinking positively or surface-level work, uses exposure, behavioral experiments, and direct work on avoidance.
- May not be enough alone for panic with agoraphobia, co-occurring depression blocking engagement, or active safety concerns.
How Cognitive Behavioral Therapy Works for Anxiety
CBT has two halves that work in tandem. The cognitive piece identifies and tests the thoughts that fuel anxiety. Cognitive restructuring is the process of examining whether a worried prediction holds up to evidence rather than treating it as fact.
The behavioral piece changes the avoidance and safety behaviors that keep the anxiety loop going. Exposure means gradually facing what the anxiety wants the person to avoid; behavioral experiments are small real-world tests of whether the feared outcome actually happens.
Combining the two is what produces durable change. Anxiety is maintained by both the catastrophic interpretation and the avoidance that prevents the interpretation from being corrected. Working on only one side typically produces partial or unstable results. Working on both, testing the predictions while reducing the avoidance, is what gives CBT its evidence base across anxiety disorders.
CBT is structured and collaborative. Each session has an agenda, and patients leave with something specific to practice between sessions.
What to Expect in a CBT Session
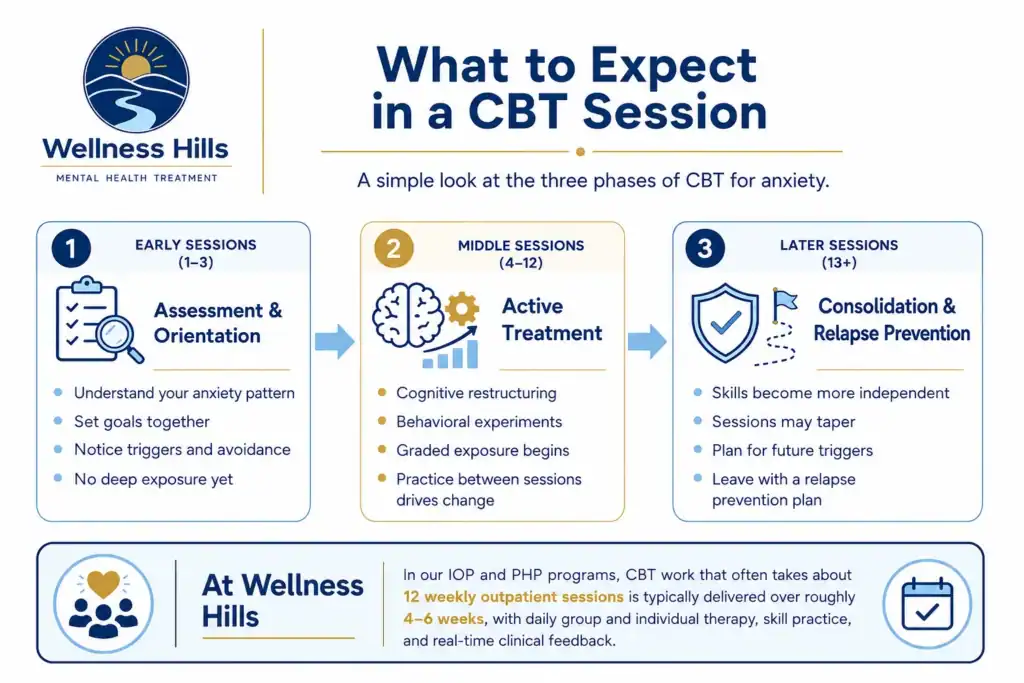
What to expect in CBT depends on the phase. The standard course has three: assessment, active treatment, and consolidation.
Early sessions (1-3): The first sessions focus on assessment and orientation rather than deep symptom work. The therapist gathers detailed history, maps how your specific anxiety operates, and explains the cycle keeping it active, often by drawing out a personalized maintenance diagram. You and the therapist set goals collaboratively. Between sessions, you start noticing patterns: triggers, avoidance, what makes the anxiety spike. No deep exposure yet.
Middle sessions (4-12): This is the active treatment phase. Cognitive restructuring, behavioral experiments, and graded exposure begin in earnest. Between-session practice becomes the engine of change; the session is for review, troubleshooting, and planning the next step. Symptom change accelerates here. It’s also where many patients want to quit, exposure feels worse before it gets better, and a good clinician addresses that directly.
Later sessions (13+): The therapist gradually hands the wheel over. Cognitive and behavioral skills are consolidated, session frequency begins to taper, and the focus shifts to relapse prevention, anticipating potential triggers for symptom recurrence and what to do if they occur. A good course of CBT ends with a written relapse prevention plan you can use to self-deliver the skills after treatment ends.
At Wellness Hills, the clinical work that typically unfolds across 12 weekly outpatient sessions is delivered over roughly 4-6 weeks in our IOP and PHP programs, where group and individual therapy run daily, and skills are practiced and reviewed with real-time clinical feedback.
What CBT Targets in Different Types of Anxiety
CBT isn’t a single protocol. What gets targeted depends on which anxiety subtype is present, and the most effective interventions vary by subtype too.
CBT for Generalized Anxiety Disorder (GAD)
CBT for generalized anxiety disorder targets chronic worry chains, intolerance of uncertainty, and the belief that worry is protective. Interventions include worry postponement (scheduling worry for a defined window), probability estimation (assessing how likely the feared outcome is), and cognitive defusion (treating worried thoughts as mental events rather than facts).
| Anxiety Pattern | What CBT Targets | Primary CBT Tools |
|---|---|---|
| Generalized Anxiety Disorder (GAD) | Chronic worry chains, intolerance of uncertainty | Worry postponement, probability estimation, cognitive defusion |
| Panic Disorder | Catastrophic misinterpretation of body sensations | Interoceptive exposure, cognitive restructuring |
| Social Anxiety Disorder | Self-focused attention, post-event rumination, safety behaviors | Video feedback, behavioral experiments, and attention training |
| Health Anxiety (Illness Anxiety Disorder) | Symptom-checking, reassurance-seeking, catastrophic medical interpretation | Response prevention, cognitive restructuring |
| Specific Phobia | Avoidance of the feared object or situation | Graded in vivo exposure |
CBT for Panic Disorder
CBT targets catastrophic misinterpretation of body sensations, the leap from “my heart is racing” to “I’m having a heart attack”, plus the avoidance and safety behaviors that prevent disconfirmation. The defining intervention is interoceptive exposure: deliberately inducing sensations such as dizziness, breathlessness, or a rapid heartbeat during the session.
CBT for Social Anxiety Disorder
CBT targets self-focused attention (excessive self-monitoring during interactions), post-event rumination (replaying interactions afterward), and the safety behaviors that maintain the belief of being negatively evaluated, over-rehearsing, avoiding eye contact, and pre-emptive apologies. Video feedback (reviewing recordings to challenge predicted versus actual performance) and behavioral experiments are core.
CBT for Health Anxiety (Illness Anxiety Disorder)
CBT targets symptom-checking, reassurance-seeking, and the cognitive bias toward catastrophic medical interpretation, the leap from a normal headache to a feared diagnosis. Response prevention is central: the patient practices not Googling symptoms, not asking partners “do I look pale?”, not repeatedly checking the body.
CBT for Specific Phobias
CBT for specific phobias relies primarily on graded exposure, systematically approaching the feared object or situation, starting at a tolerable intensity and working up. Cognitive work is supportive but secondary. Specific phobias have the strongest evidence base for short-course CBT, with focused protocols well supported by research.
A good CBT clinician adapts the protocol to the subtype; there’s no single template, and treating panic the way one would treat GAD misses the point of the modality.
Common Misconceptions About CBT
A few misreads about CBT come up repeatedly. They’re quiet objections that delay engagement or color your expectations of a course of treatment. Each is reasonable on its face. None survives close contact with what CBT actually involves.
“It’s just positive thinking.” CBT doesn’t replace negative thoughts with positive ones; it tests whether the anxious prediction holds up to evidence. The answer is often “the feared outcome is unlikely but possible, and I could cope with it.” That’s accuracy, not positivity.
“It’s too surface-level; it doesn’t address root causes.” CBT does work with deeper material when clinically relevant. Core beliefs, schemas, and trauma-informed adaptations are part of the toolkit. The assumption that insight is necessary for change isn’t well-supported by outcomes research: behavioral change frequently produces the cognitive shift, not the other way around.
“Homework is busywork.” Between-session practice is where change happens. Sessions plan and review; practice is the active ingredient. Patients who skip the homework don’t improve at the expected rate, and most CBT clinicians will name this directly, not as judgment, but as clinical information.
“It won’t work for severe anxiety.” CBT is the most extensively researched psychotherapy for panic disorder, GAD, and social anxiety. A first-line guideline recommendation even for severe presentations. OCD calls for the ERP variant; PTSD, for trauma-focused CBT or CPT, not generic CBT. Severe anxiety often requires more intensive delivery (IOP/PHP) and sometimes medication support, not a different therapy.
“Exposure is dangerous or retraumatizing.” Exposure is graded, collaborative, and never coerced. A patient never does exposure work they haven’t consented to and aren’t prepared for. Done correctly, exposure is uncomfortable but not traumatic, and the discomfort is the mechanism, not a side effect.
What Improves First, and What Takes Longer
Early gains (weeks 1-3): Many patients report better sleep, reduced anticipatory dread, and a clearer understanding of what’s happening to them. Psychoeducation alone reduces the secondary anxiety of being anxious about anxiety.
They don’t yet feel less anxious in feared situations, but they understand their anxiety, which is itself stabilizing. For patients with chronic anxiety and entrenched physical symptoms, somatic gains often take longer than this early window; somatic relief shouldn’t be the metric for whether treatment is working.
Mid-range gains (weeks 4-8): Avoidance starts breaking down. Patients re-enter situations they’d been avoiding, driving, social events, work meetings, and notice the feared outcome didn’t happen, or wasn’t as catastrophic as predicted.
Cognitive flexibility improves; worry chains shorten. Panic attacks, if present, typically become less frequent and less catastrophically interpreted when they do occur. This is the window where most of the visible symptom change accumulates.
Slower-changing gains (weeks 8+): Core beliefs, “I’m fundamentally vulnerable,” “I can’t handle distress”, shift last. Physical symptoms like chronic muscle tension, GI complaints, and fatigue often lag behind cognitive and behavioral change. Confidence that the anxiety won’t return takes the longest, which is part of why relapse prevention planning is built into the later sessions.
What should worry you if it’s not moving: If a patient is 6-8 weeks in and not seeing reduced avoidance or reduced frequency of feared episodes, that’s a clinical signal, not a reason to quit, but a reason for the clinician to re-formulate.
Common causes include subtle ongoing avoidance (the patient is technically doing exposure but using safety behaviors that block disconfirmation), untreated co-occurring depression, alcohol or cannabis use undermining exposure work, or a level-of-care mismatch.
A clinician who keeps running the same protocol at week 10 without reformulating it is missing the diagnostic information that stuckness provides.
How Progress in CBT Is Tracked
Progress in CBT should be measurable, not just felt. A clinician working from current standards tracks two parallel data streams: standardized symptom scales and functional markers.
Standardized scales include the GAD-7 for generalized anxiety symptoms, the PHQ-9 when depression is co-occurring or suspected, the PCL-5 when trauma symptoms are present, and a panic disorder severity scale when panic is the primary presentation. These are administered at baseline and re-administered at regular intervals, every 2-4 weeks in most outpatient courses, sometimes weekly in IOP or PHP. The Columbia Suicide Severity Rating Scale (C-SSRS) is added when symptoms suggest risk.
Functional markers track how symptoms affect the patient’s life: avoidance behaviors, sleep quality, work or school attendance, panic frequency, time spent worrying, frequency of reassurance-seeking, and participation in valued activities. A patient whose GAD-7 score is dropping but whose avoidance hasn’t shifted is sending different clinical information than one whose score is stable but whose functional engagement is climbing.
The clinical decision point is built into the data, not added later. If standardized scores aren’t moving and functional markers aren’t improving after 6-8 weeks, that’s the signal to re-formulate, not to repeat the protocol harder. Common causes of measurable stuckness include subtle safety behaviors that block exposure from doing its work, untreated co-occurring conditions, a level-of-care mismatch, or substance use that undermines between-session practice.
Measurement-based care also makes the treatment endpoint visible. A patient and clinician can see when symptoms have remitted enough to shift from active treatment to relapse prevention, and when continued weekly therapy is no longer producing additional gain. At Wellness Hills, GAD-7 and PHQ-9 are part of routine clinical monitoring across IOP and PHP.
Core CBT Techniques Used for Anxiety

The core CBT interventions for anxiety include several distinct techniques and exercises, used in combination based on the formulation.
Cognitive restructuring identifies, tests, and revises anxious predictions, examining whether they hold up to evidence. Behavioral experiments are collaborative, real-world tests of feared predictions, designed with the therapist, run by the patient between sessions to gather data that discussion alone can’t generate.
Graded exposure comes in three variants: in vivo (real-world contact), imaginal (engaging with the feared scenario in the mind), and interoceptive (inducing the bodily sensations the patient fears).
Worry postponement and stimulus control, confining worry to a scheduled window, are central in GAD. Activity scheduling builds in valued and reinforcing activity when co-occurring depression has collapsed behavior. Attention training redirects self-focused or symptom-focused attention outward, useful in social anxiety and health anxiety.
Relaxation techniques are used selectively rather than reflexively. For panic disorder, relaxation can become a safety behavior that prevents the patient from learning that their body is safe without it. Many clinicians de-emphasize or even target relaxation for elimination in panic-focused CBT.
Techniques are sequenced to the formulation, not run through a menu. A patient whose treatment looks like a worksheet packet isn’t getting CBT; they’re getting CBT-flavored homework.
Compared to Other Anxiety Treatments
CBT is the most extensively researched psychotherapy for anxiety, but it isn’t the only evidence-based option. Several other modalities are well supported, and the right treatment is sometimes a combination rather than a single choice.
Acceptance and Commitment Therapy (ACT) is a related modality that shares CBT’s emphasis on behavioral change but de-emphasizes symptom reduction in favor of psychological flexibility, the ability to act in line with personal values even when anxious thoughts and sensations are present. ACT has solid research support for generalized anxiety, social anxiety, and panic, and is often a reasonable fit for patients who haven’t responded to standard CBT or whose anxiety is bound up with broader life direction questions.
Mindfulness-Based Cognitive Therapy (MBCT) integrates mindfulness training into a CBT framework. Its strongest evidence is in relapse prevention after acute treatment, particularly for patients with recurrent depression alongside anxiety. It tends to work better as a sequel to acute-phase treatment than as a standalone first-line intervention.
Medication is often used alongside CBT rather than instead of it. Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) are first-line pharmacotherapy for most anxiety disorders, with evidence for sertraline, escitalopram, paroxetine, venlafaxine, and duloxetine across various subtypes.
Benzodiazepines are sometimes used short-term but aren’t a first-line maintenance treatment for anxiety. A psychiatric provider at Wellness Hills, Paula Weisman, PMHNP-BC, determines whether medication is appropriate, which agent fits the symptom profile, and how it’s coordinated with therapy.
Two CBT variants deserve specific mention. Exposure and Response Prevention (ERP) is the indicated treatment for OCD and OCD-spectrum presentations, not generic CBT. Trauma-focused CBT (TF-CBT) and Cognitive Processing Therapy (CPT) are the indicated treatments for PTSD. A clinician trained in standard CBT for anxiety isn’t necessarily trained in ERP or TF-CBT; if OCD or PTSD is the primary presentation, the patient needs a clinician with the matching specialty training.
Self-Guided CBT vs. Working With a Therapist
Yes, with limits. Self-guided CBT, well-established books, structured workbooks, and digital CBT programs can produce real benefit for mild-to-moderate anxiety, particularly if you have the discipline to do the practice consistently. The research support for digital CBT is reasonable, and the cost and access advantages are real.
The limits matter. For moderate-to-severe anxiety, panic with significant avoidance, or anxiety that hasn’t shifted on a self-guided attempt, a clinician produces meaningfully better outcomes. Exposure work, the active ingredient in most anxiety subtypes, is hard to design and execute alone, and a clinician catches subtle safety behaviors you can’t see in yourself.
A reasonable middle path is to try a structured, self-guided program for 4-6 weeks. If avoidance is meaningfully shifting, keep going. If not, that’s data; working with a clinician is the next step.
How Clinicians Decide Whether CBT Is the Right Fit
CBT is well-supported for most anxiety presentations, but the assessment that determines whether it’s the right starting point and at what level of care is more nuanced than “do you have anxiety.” At Wellness Hills, the clinical decision rests on six factors.
First, the presenting anxiety pattern. Worry-driven anxiety, panic with feared body sensations, social fear with avoidance, checking and reassurance-seeking, and trauma-driven anxiety each call for different CBT adaptations. The pattern shapes the protocol.
Second, functional impairment. The clinician assesses how the anxiety is affecting work, school, caregiving, sleep, and daily activities. A patient who is symptomatic but functioning has different treatment needs than one whose avoidance has collapsed major life domains.
Third, safety screening. Active suicidal ideation, recent self-harm, or current crisis-level symptoms change the immediate next step. Outpatient CBT may not be the appropriate first step; a higher-acuity evaluation should come first.
Fourth, co-occurring conditions. Untreated depression, active substance use, OCD-spectrum symptoms, bipolar features, or psychotic symptoms each shape whether standard CBT for anxiety is the right protocol or whether a different sequence of care is indicated.
Fifth, capacity for between-session practice. CBT relies on the patient completing exposures and experiments between sessions. A patient whose work schedule, caregiving demands, or symptom severity make that impossible may need a more intensive level of care delivered with clinical support.
Sixth, baseline measurement. GAD-7, PHQ-9, brief functional history, and relevant subtype-specific scales establish a baseline against which subsequent sessions can be tracked. Without baseline measurement, progress is impossible to evaluate objectively.
This assessment usually takes one to two sessions. The output isn’t only a diagnosis; it’s a recommendation about the right level of care, the appropriate CBT adaptation, and whether medication evaluation or treatment for a co-occurring condition should be added concurrently.
When Weekly CBT Is Enough and When It Isn't
Weekly CBT therapy for anxiety is typically enough when anxiety is moderate, daily functioning is intact, between-session work is feasible, severe co-occurring depression or substance use isn’t blocking engagement, and the patient isn’t in acute crisis.
Consider a higher level of care when avoidance has collapsed daily functioning, panic with agoraphobia keeps you housebound, weekly therapy has been tried adequately without movement, or daily clinical contact is needed.
CBT isn’t always the first move. When anxiety is connected to active safety concerns, severe substance use, mania or psychosis, or medical instability, the first step isn’t standard outpatient CBT; it’s a higher-acuity evaluation.
At Wellness Hills Mental Health in Chester, NJ, our PHP and IOP programs deliver CBT-informed individual and group therapy multiple days per week, compressing what weekly therapy would span over months.
IOP runs in two tracks: a 3-evening schedule (Monday/Tuesday/Thursday, 6-9pm) for working patients, and a 5-morning track (Monday-Friday, 9am-12pm). PHP runs six days a week for the most concentrated clinical contact short of inpatient.
Frequently Asked Questions
The questions below are the ones most patients ask before starting CBT or when deciding whether to escalate from weekly therapy to a higher level of care.
How long does CBT for anxiety usually take?
Twelve to twenty weekly sessions is the standard outpatient course for most anxiety presentations. Specific phobias can be shorter; complex presentations may run longer. In IOP and PHP at Wellness Hills, the same clinical hours are typically delivered over 4-8 weeks.
Does CBT work for panic attacks or severe anxiety?
Yes. CBT has strong research support for panic disorder, including severe cases. Severe presentations often respond better to intensive delivery (IOP or PHP) than to weekly therapy, but the treatment is the same CBT, with interventions like interoceptive exposure.
Can CBT be combined with medication?
Yes. Many patients with moderate-to-severe anxiety benefit from medication management alongside CBT. A psychiatric provider can determine whether medication is appropriate and which option fits the person’s symptoms, history, and safety profile. The two approaches work differently and aren’t mutually exclusive.
What if CBT didn't work for me before?
A non-response to CBT is clinical information, not a verdict. Common causes include subtle ongoing avoidance, a level-of-care mismatch, untreated co-occurring conditions, or a clinician who didn’t adapt the protocol to your anxiety subtype. Re-formulating with a new clinician, sometimes at a higher level of care, often produces different results.
How do I know if CBT is working for me?
Look for four signals: less avoidance of situations you’d been steering around, fewer safety behaviors during exposure, better participation in work and daily life, and improved tolerance of uncertainty without immediately seeking reassurance. Standardized scales like the GAD-7 should also trend downward over a 6-8-week window. Subjective “feeling less anxious” is lagging; behavioral and scale changes move first.
What happens if exposure makes my anxiety worse at first?
Temporary discomfort during exposure is expected and part of the mechanism; it’s how the nervous system learns that the feared outcome won’t happen. Exposure should always be planned, consent-based, and titrated with the clinician; you shouldn’t be doing exposures you haven’t prepared for. If anxiety is worsening between exposures and not resolving, that’s clinical information that calls for the clinician to re-formulate, not for you to abandon the work.
When should someone consider IOP instead of weekly CBT?
Consider IOP when avoidance is collapsing functioning in major life domains, when weekly therapy has been tried for 6-8 weeks without movement, when panic with agoraphobia is keeping you housebound, when co-occurring depression or substance use is blocking engagement with weekly work, or when multiple clinical contacts per week are needed to make progress. PHP applies when the same concerns are more severe and a daily clinical structure is needed.
Clarifying Your Next Step
If you’ve been doing weekly therapy without the progress you expected, or you’re trying to figure out whether you need more than weekly care to get traction, a clinical assessment can clarify the right next step. Wellness Hills offers confidential assessments to help you determine whether outpatient care, IOP, or PHP is the right fit.
You can request an assessment, verify your insurance, or talk with admissions; there’s no obligation to enroll, and a good assessment is useful regardless of where you go for care.
Sources:
American Psychological Association (APA) | Evidence-Based Practice in Psychology – Professional psychology resource explaining evidence-based practice as the integration of best available research, clinical expertise, and patient characteristics, culture, and preferences.
Hofmann et al. | The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses – Peer-reviewed review summarizing meta-analytic evidence for cognitive behavioral therapy across psychiatric conditions, including anxiety disorders.
Kazantzis et al. | Quantity and Quality of Homework Compliance: A Meta-Analysis of Relations With Outcome in Cognitive Behavior Therapy – Peer-reviewed meta-analysis examining the relationship between CBT homework completion, homework quality, and treatment outcomes.
Andrews et al. | Computer Therapy for the Anxiety and Depression Disorders Is Effective, Acceptable and Practical Health Care: An Updated Meta-analysis – Peer-reviewed meta-analysis evaluating internet-delivered and computer-based CBT for anxiety and depressive disorders.
Editorial Standards
Our Editorial Policy
Our editorial standards keep our mental health content accurate, compassionate, and evidence-informed. Articles are developed using credible sources, reviewed for medical accuracy when needed, and regularly updated.